
Is Your Hypermobility Causing Pelvic Floor Problems? What the Science Says
Part 1: The Connection
Welcome! This is Part 1 of a 2-part series on the important (and yet misunderstood) relationship between hypermobility and pelvic health. Scroll through this first to better understand the connection - and then head over to Part 2 for some action items and evidence-based exercises to get started on healing.
Summary, or tl;dr section
Hypermobility is a term describing having more flexible, or less stiff, joints and connective tissue than other people. It exists on a spectrum, meaning some people feel mild effects while others feel much more impact. It’s common for people with hypermobility to have overactive pelvic floor muscles. This blog talks about why this happens, how it could impact strength and function, and how you might know you’re having pelvic floor issues.
Throughout the blog you’ll find links to the most recent evidence on hypermobility and the pelvic floor, all synthesized in one place with links for you to review if you’d like to read them for yourself. With the right support and guidance, even the most bendy of us can find pelvic floor stability. Stay tuned for part 2 for action items and evidence-based exercises.
A little disclaimer before we go on: gentle reminder that this blog is solely for your information from an expert in scoliosis and pelvic health. This blog is for general information only and can not serve as medical advice. Each person will have different circumstances and you should ask your personal medical & wellness team, or you can book a consult for personalized expert advice.
As a pelvic floor and scoliosis specialist, I see many patients and virtual clients with hypermobility. Here are some of the most common questions I get:
"Can hypermobility cause pelvic floor dysfunction?"
"Why is my pelvic floor tight if I have EDS/ generalized joint hypermobility?"
"What are the symptoms of pelvic floor problems with hEDS?"
This blog is part 1 in a 2-part series to break it down into small, digestible segments, to help you understand the connection, what to look for and how to find relief if you’re struggling.
So let’s dive in.
Hypermobility & Your Pelvic Floor: Why It Happens
You may find yourself your joints move more than most people’s. For many people, it feels as though your body is extra bendy, although for some people they just feel stiff.
This can also be described as hypermobility, which is a term describing someone with excessive movement in their joints. Hypermobility is often a genetic issue with the collagen in the connective tissue, or fascia. Having less stiffness in your connective tissues and joints can mean your muscles have to work extra hard to keep you steady.
This lack of stiffness also affects your pelvic floor. Those muscles sit at the bottom of your pelvis and work to stabilize you, allow you to go to the bathroom (or hold it when you can’t), help support your organs, and support your movement.
Our pelvic floor is often referred to as the “floor of our core”, which I discussed at length in this blog on the pelvic floor. The demands we place on our bodies require a dynamic system of pressure management. A weakness anywhere in this deep core system can cause pain and dysfunction. Think of how easily you can crush an empty soda can versus a sealed one filled with liquid. The walls may be relatively thin, but the pressure is what gives the can strength.
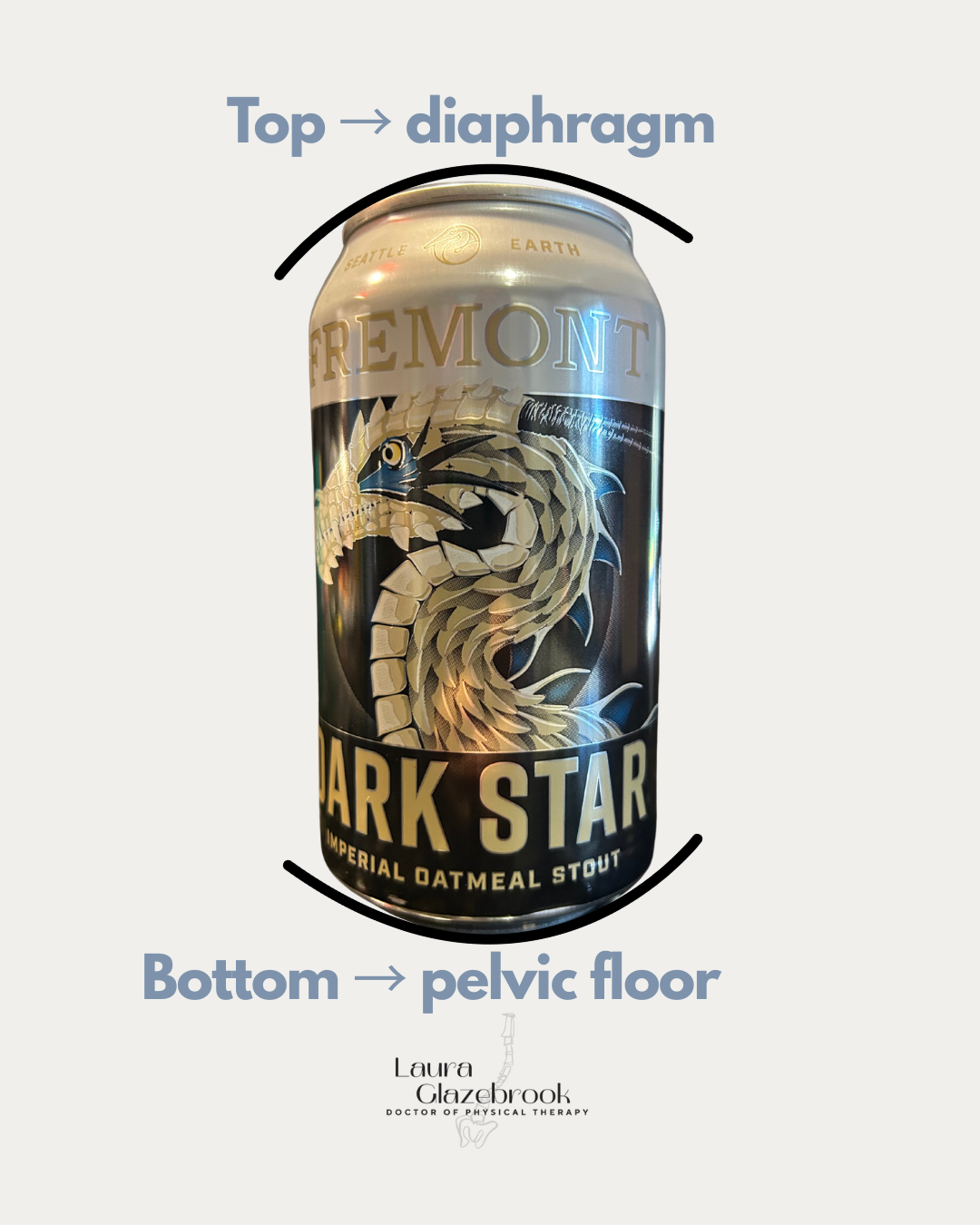
Check out this graphic I made for an Instagram post discussing this concept further. Check it out!
If you have hypermobility, the tissues in your body are stretchier, or less stiff, than someone without it. That includes the fascia and ligaments in your pelvic floor. This lack of support can cause overactivity in your muscles, leaving them feel tired, tight, or even painful.
Common issues people with hypermobility & pelvic floor overactivity experience are:
Pressure or heaviness deep within the pelvis
Leaking pee or difficulty holding your poo or gas
Constipation, feeling unable to empty your bowels
Discomfort or pain with intimacy, or being unable to climax
Feeling pain deep inside your pelvis, genital region, low back or deep hips
If this is describing you, that means your body needs a little extra support.
The lack of stability can be particularly problematic for our core canister and the structures that make up our pelvis. The pelvis is designed to be our basis of stability, and is made up of two strong bones that connect to the sacrum and the spine.
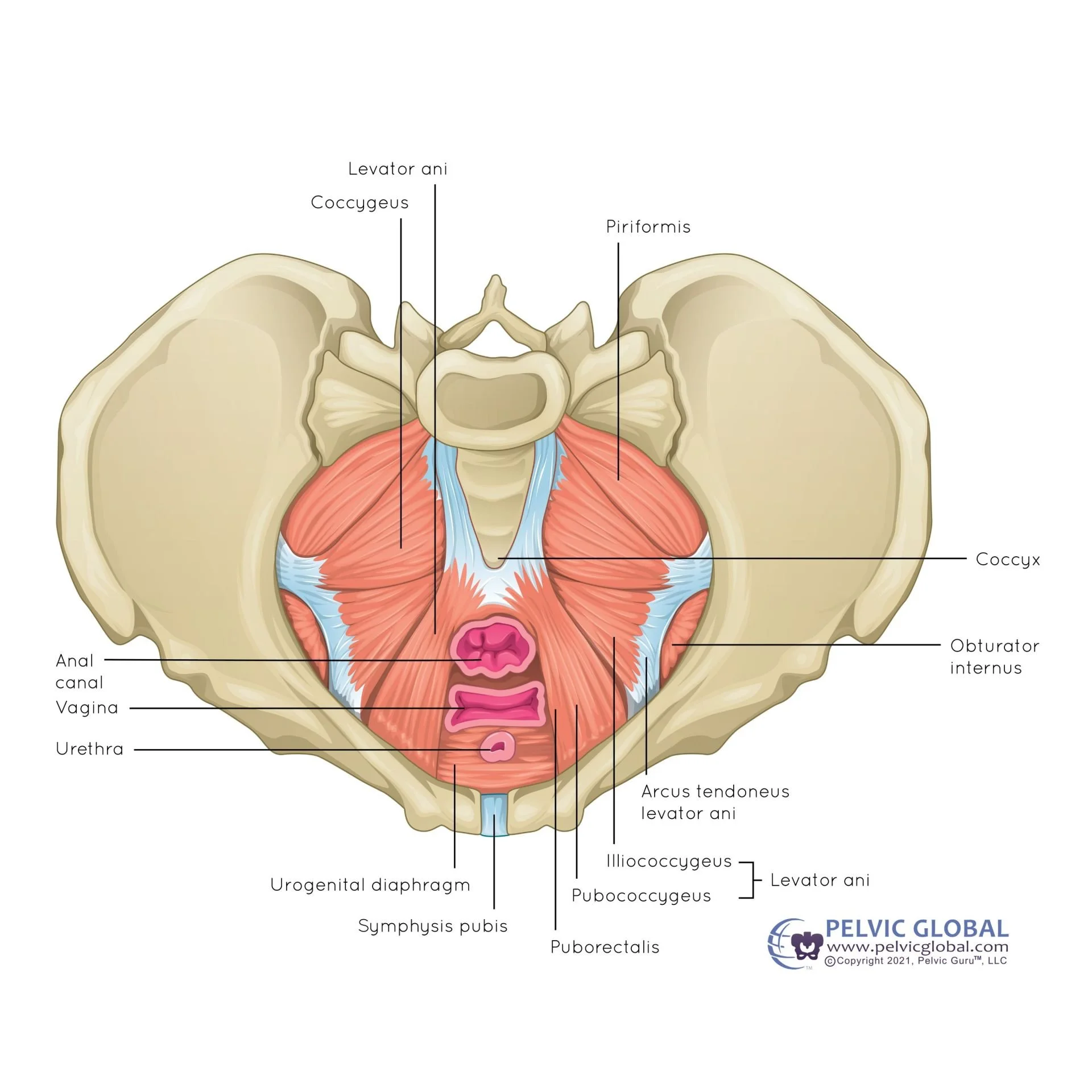
Here’s a view of the pelvis bones, looking from above, with the connections to the spine bones at the top of the picture and the sling of muscles at the base of the pelvis.
Our pelvic anatomy, along with the ligaments and connective tissue, is responsible for connecting our trunk to our legs and supporting our weight as we stand, walk, and move day to day.
The trouble is, our bodies rely on a certain amount of tension and stability to hold us up. When we lack the support of our connective tissues, our muscles have to work overtime to compensate for tasks ranging from walking all the way to high performance sports. When any of those stabilizing “walls” aren’t doing their job, we often feel the worst of the effects in the pelvic floor, which will tighten and become overactive. This can lead to a lot of issues like pelvic pain with movement, intercourse or bowel movements, changes in sexual function, or urinary leakage.
But don’t worry! With the right support, your pelvic floor can feel strong, stable, AND mobile again.
But first, let’s talk a bit more in depth about hypermobility and its impact on the pelvic floor.
What is hypermobility?
According to the Hypermobility Syndromes Association, hypermobility is basically defined as any condition in which joints and tissues within your body that bend more than they should.
Hypermobility exists on a spectrum, meaning some people are more severely impacted than others. Additionally, perhaps people have some areas or joints that are extra bendy than others. There are some types of Ehlers Danlos Syndrome that even affect the stability of blood vessels and organs, and can be quite debilitating.
Someone can have asymptomatic or symptomatic hypermobility - that basically means that they may feel the effects of their overly loose or flexible joints and connective tissues, or they may not.
*Some* types of hypermobility:
Hypermobile spectrum disorders (HSD) & generalized joint hypermobility(GJH)
Ehlers Danlos Syndrome (EDS) - a group of conditions created by genetic alterations in collagen
Marfan Syndrome (MFS) - skeletal abnormalities as well as heart and lung defects
Pseudoxanthoma elasticum - affecting the skin, arteries, and eyes
Osteogenesis imperfecta - characterized by fragile bones & teeth
This is by no means an exhaustive list, but gives you an idea on the different types and how you may look different from someone else that also has hypermobility.
Did you know?
|
Did you know? |
As a quick aside: did you know that people with hypermobility are also more prone to developing scoliosis? Read more about scoliosis here!
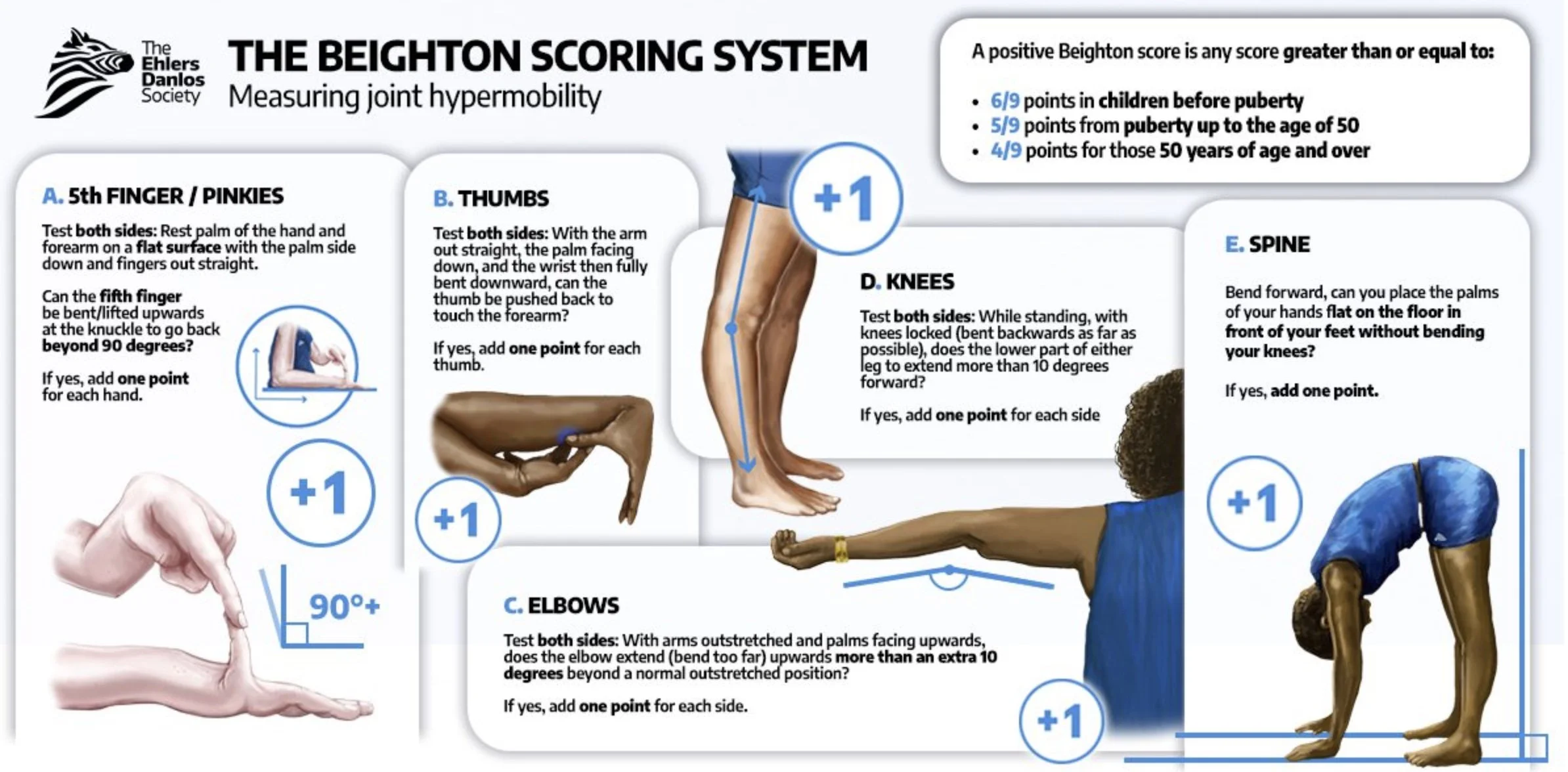
Check out this infographic on screening for joint hypermobility. Click the image to visit the EDS website!
How hypermobility impacts your daily life
Again, since there’s such a wide variety of how affected someone can feel with hypermobility and the effects, this can look very different for you than it does for someone else. Depending on the type of hypermobility and the severity, you may feel incredibly impacted or you may feel minimally impacted.
You may notice your muscles feel tired after short periods of time, holding yourself up against gravity (think sitting without back support or standing for a period of time)
Some things you may notice with hypermobility:
Decreased body awareness - also called proprioception, people with hypermobility syndromes can find it hard to know where their body is in space at any given time. This has been suggested as a common issue in hypermobility in this 2015 Finnish study. This can look like:
Feeling clumsy, bumping into furniture or doorframes
Tripping over your feet, particularly on stairs or uneven surfaces
Trouble coordinating fine movements like threading a needle
Dropping objects or fumbling with your fingers
Repetitive joint or muscle injuries - it’s common to experience persistent ankle sprains, shoulder dislocations, hyperextending knees, elbows and fingers
Widespread or persistent pain - people with connective tissue deficits can suffer with pain in more than one area of the body, which can impact ability to do more strenuous tasks like lifting, doing certain types of exercise, et cetera
Balance challenges - lack of stiffness in the connective tissues can also look like difficulty balancing on one leg, or on uneven surfaces like gravel, grass or sand
Dizziness - it is common to experience dizziness, lightheadedness or something called dysautonomia with hypermobility conditions. Check out this 2025 article investigating the link between dizziness and joint hypermobility on NIH!
Decreased stamina - people with hypermobility can often find prolonged standing, walking or more strenuous tasks to be more tiring, needing more frequent rest breaks because of the increased muscle effort needed to hold them up
How hypermobility affects your pelvic floor
So how does this present itself below the belt?
Here’s your disclaimer that, just as every person living with hypermobility may have different symptoms, not everyone with hypermobility will experience the same pelvic floor effects.
When we lack stiffness in the connective tissues that normally provide our postural support, it means the muscles have to take up more of the slack. When we’re looking at a complex system like the pelvic floor muscles, that increased demand can lead to overactivity, or over-working, of those muscles.
Again, as I mentioned earlier, this can present differently in different people. Keep reading…
When the Muscles Compensate
Pelvic floor “gripping” is common in those of us with hypermobility. This can feel like:
Chronic tension or pressure
Pain in the pelvis, groin or tailbone
Constipation
All that in mind, one thing I want you to remember: just because the muscles are overactive, doesn’t mean they are strong! More often than not, they are functionally weak - meaning, they stay contracted in a very small range of motion, never moving up or down.
Having a hard time with that concept? Think about muscles in other areas of the body: we want to be able to activate our biceps if our arms are mostly bent, halfway bent or mostly straight. If we can only turn that muscle on in certain positions, that can be a problem.
The Stability Chain Changes
The lack of stability can be particularly problematic for our core and the structures that make up our pelvis. The pelvis is designed to be our basis of stability, and is made up of two strong bones that connect to the sacrum and the spine. Its anatomy, along with the important collection of ligaments, are responsible for connecting our trunk to our legs and supporting our weight as we stand, walk, and move about our daily lives.
When any of those “walls” that should stabilize us aren’t doing their job, it’s quite common to see the worst of the effects occur on the pelvic floor, which will tighten and become overused. This can lead to a lot of issues like pelvic pain with movement, intercourse or bowel movements, changes in sexual function, or urinary leakage.
The pelvis is the center of your whole body
Hypermobility changes how your trunk and legs support you
This can lead to:
Hip shifting
Poor load transfer
Tipping forward/backward when standing
Our pelvic floor is often referred to as the “floor of our core”, which I discussed at length in a previous blog post. The demands we place on our bodies require a dynamic system of pressure management. A weakness anywhere in this deep core system can cause pain and dysfunction. Think of how easily you can crush an empty soda can versus a sealed one filled with liquid. The walls may be relatively thin, but the pressure is what gives the can strength.
Common pelvic floor concerns with hypermobility
It’s actually very common for people, particularly women, dealing with the effects of hypermobility to experience pelvic pain and instability. Commonly they report more issues surrounding pregnancy and the postpartum period.
That can look like:
Leaking with laughing/exercise
Heaviness or pressure
Pain with sex
Constipation
Hip/pelvic instability
Feeling chronic, constant low back and pelvic tension
Trouble finding “neutral” posture
A related note on hypermobility and the pelvic floor: there is some evidence to suggest that there is a relationship between hypermobility and developing pelvic organ prolapse (referencing this 2015 study), as well as some older research on EDS and urinary leakage, but nothing definitive and certainly as I’ve mentioned before, having a link doesn’t mean one thing causes the other. Understanding research and the implications are key!
Key points from the most recent research to date
A 2015 study polled 325 Flemish physiotherapists to determine their knowledge/ confidence in treating those with hypermobility disorders and found them to have weak knowledge overall — anyone living in the U.S. at least could agree that it’s an area where healthcare providers need more training and competence!
This 2014 study investigated the complex relationship between generalized joint hypermobility and pelvic floor dysfunction related to childbirth & obstetric outcomes. Based on 46 of the women with hypermobility, there was no significant increase in pelvic floor dysfunction within the first 10 years postpartum; however, the authors did highlight the complexity of pelvic floor dysfunction. Interestingly, they also noted that it’s possible that because the women in the study were younger (average age 40), they would not experience pelvic floor dysfunction until later in life.
A systematic review on Ehlers Danlos Syndrome from 2019 determined there was a relatively high prevalence of urinary, gynecological and obstetrical disorders in the EDS population (ranging from 25 to 41%) after amassing information from 105 different studies.
This systematic review from 2022 found a well-established relationship between participants with hypermobility and decreased proprioception, or awareness of the body’s position in space, over multiple studies.
Next Steps…
If you’ve read through this and have determined you may need help, you are not alone! Here are some action steps you can take to get the help you need:
Read part 2 of the blog with some simple strategies and exercises to get you started.
Book a virtual consult with me to determine a personalized action plan to help your spine and pelvis find stability.
Seek a local pelvic PT if you have access to one. My recommendation is to find someone who lists hypermobility as a speciality within their listing.
Bottom line: it’s common to experience pelvic floor concerns with hypermobility and you’re not alone, and there’s also help to be found if you need it. You don’t need to suffer alone.
Feel free to contact me if you have specific questions or drop a comment below.
Sources & Evidence Links
Articles:
Rombaut L, Deane J, Simmonds J, et al. Knowledge, assessment, and management of adults with joint hypermobility syndrome/Ehlers-Danlos syndrome hypermobility type among Flemish physiotherapists. Am J Med Genet C Semin Med Genet. 2015;169C(1):76-83. https://doi:10.1002/ajmg.c.31434
Gilliam E, Hoffman JD, Yeh G. Urogenital and pelvic complications in the Ehlers-Danlos syndromes and associated hypermobility spectrum disorders: A scoping review. Clin Genet. 2020;97:168–178. https://doi.org/10.1111/cge.13624
Knoepp LR, McDermott KC, Muñoz A, Blomquist JL, Handa VL. Joint hypermobility, obstetrical outcomes, and pelvic floor disorders. Int Urogynecol J. 2013;24(5):735-740. https://doi:10.1007/s00192-012-1913-x
Buryk-Iggers S, Mittal N, Santa Mina D, et al. Exercise and Rehabilitation in People With Ehlers-Danlos Syndrome: A Systematic Review. Arch Rehabil Res Clin Transl. 2022;4(2):100189. Published 2022 Mar 4. doi:10.1016/j.arrct.2022.100189
Other Sources: